BAY 81-8973: Pharmacokinetic Parameters in Adolescents, Adults, and Children With Severe Hemophilia A
Introduction:
BAY 81-8973 is Bayer’s new full-length recombinant factor VIII product in development for the treatment of hemophilia A, with no human- or animal-derived raw materials added to the cell culture, purification, or formulation process. The pharmacokinetic (PK) properties of BAY 81-8973 were investigated in 3 studies in previously treated adults, adolescents, and children.
Methods:
For all PK evaluations, a single dose of 50 IU/kg BAY 81-8973 was injected. Serial blood samples were collected over 48 hours in adults and 24 hours in children <12 years of age. PK samples in adolescents and adults were analyzed using one-stage and chromogenic assays. Limited samples were collected in children and were analyzed using only the chromogenic assay. Ethnic subgroups included Chinese, Japanese, and non-Asian patients.
Results:
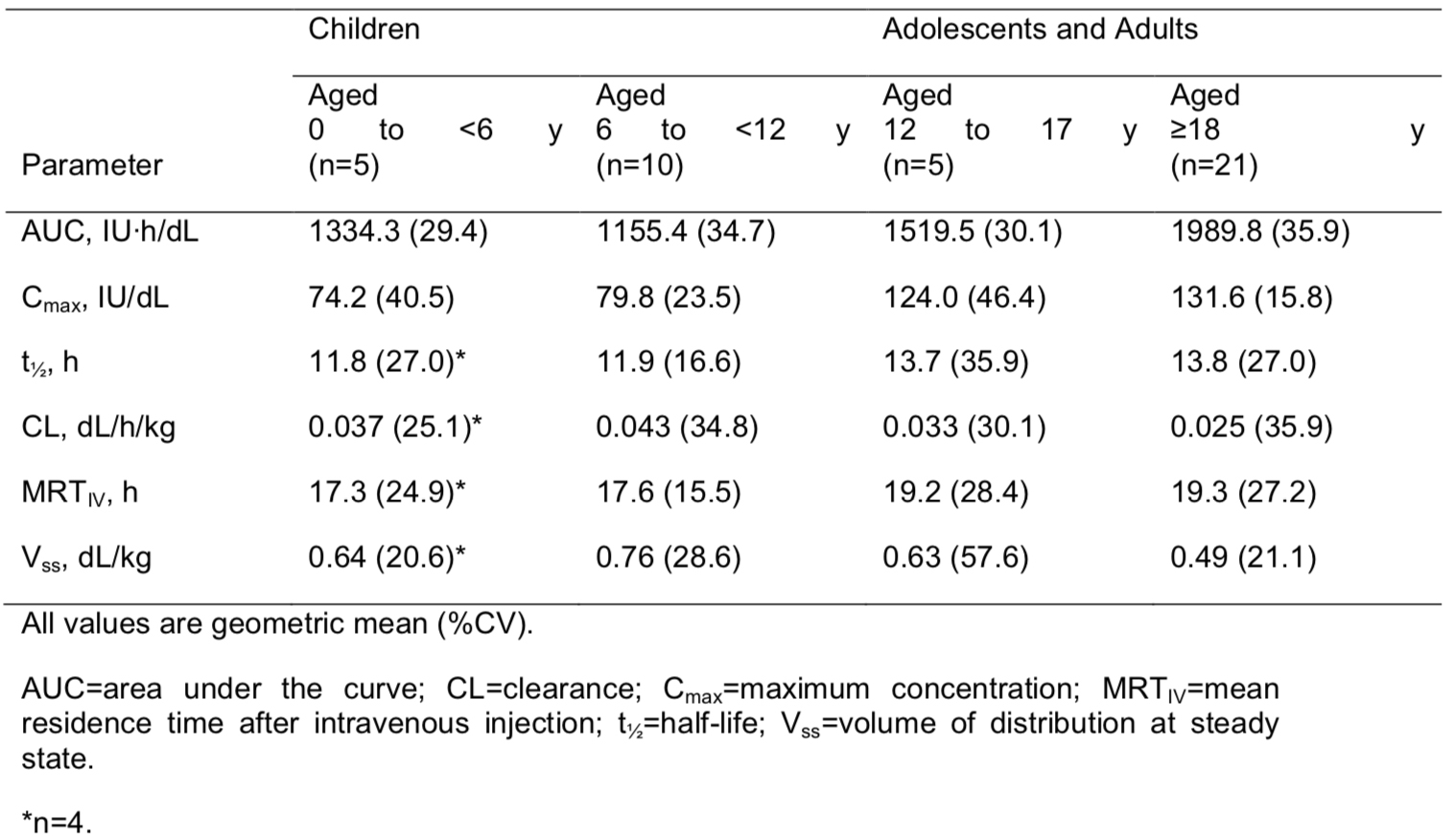
PK parameters using the chromogenic assay for children (aged <12 years), adolescents (aged 12–17 years), and adults (aged ≥18 years) are shown in Table 1.
Table 1. Pharmacokinetic Parameters Based on the Chromogenic Assay
Conclusions:
Analysis of PK across the different age groups showed that the values for maximum concentration (Cmax) and area under the curve (AUC) for adolescents were within the range of those seen for adults. PK values were slightly lower in children than in adults. There were no significant differences among the ethnic groups studied.