
An Integrated Safety and Efficacy Analysis of Sofosbuvir-Based Regimens in Patients with Hereditary Bleeding Disorders
Objective:
Patients with hereditary bleeding disorders have been included in Phase 2 and 3 clinical trials of sofosbuvir (SOF), ledipasvir/sofosbuvir (LDV/SOF), sofosbuvir/velpatasvir (SOF/VEL), and sofosbuvir/velpatasvir/voxilaprevir (SOF/VEL/VOX) as well as in a dedicated study (n = 120) in this patient population. This integrated analysis evaluates the safety and efficacy of SOF-based regimens in HCV-infected patients with hereditary bleeding disorders.
Methods:
HCV-infected patients with a medical history of a hereditary bleeding disorder who participated in a SOF-based Phase 2 or 3 study were included in this pooled analysis. Medical history term(s) used to identify patients with bleeding disorders included variations of Hemophilia A or B, Von Willebrand’s Disease, Factor Deficiencies, or conditions associated with hemophilia.
Summary:
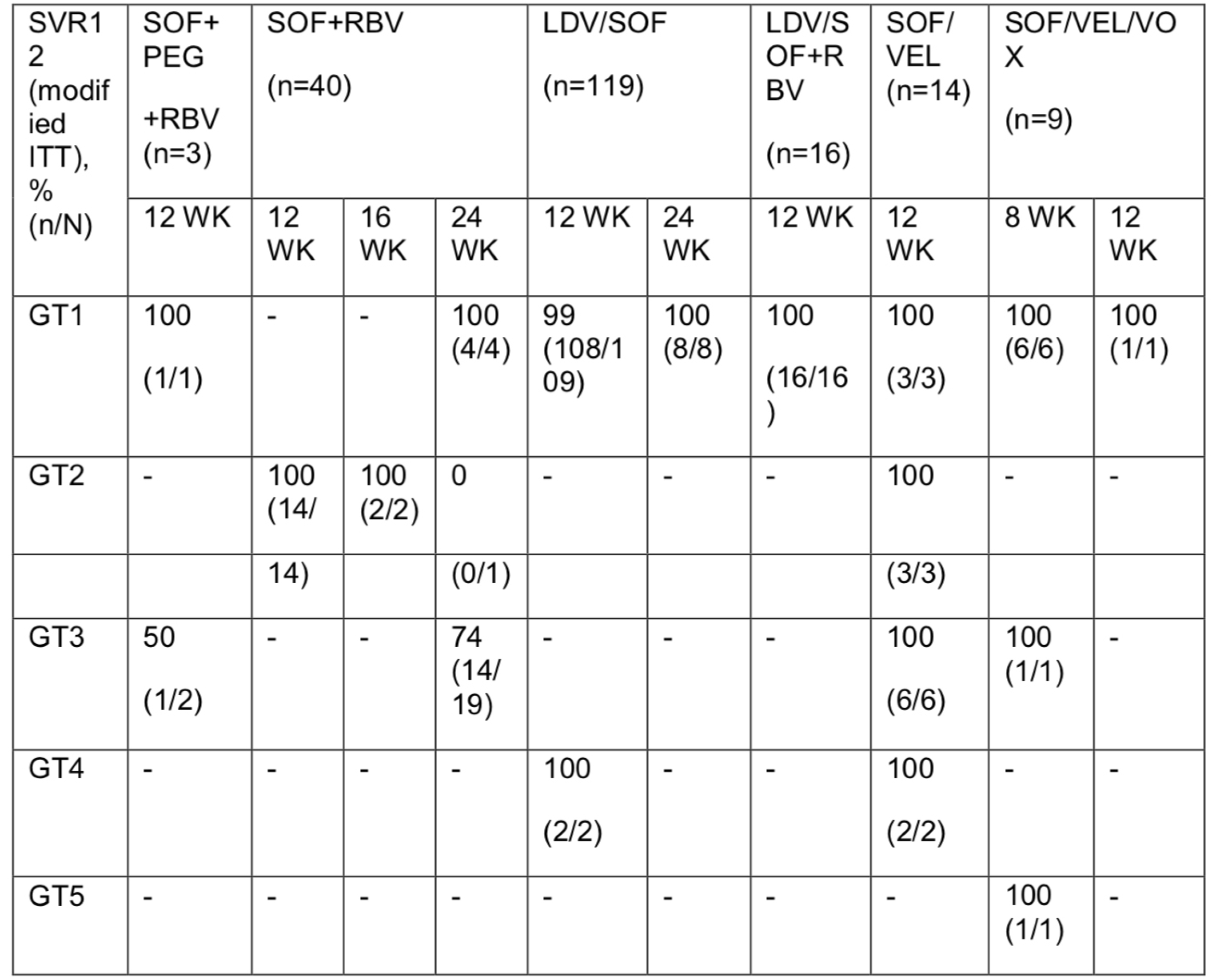
A total of 201 patients (74 GT1, 10% GT2, 14% GT3, 2% GT4, <1% GT5) with bleeding disorders were identified across 19 studies. The majority were male (91%), Caucasian (82%), IL28B non-CC (70%), HCV treatment-naïve (55%), and without cirrhosis (74%). Hemophilia A (65%) and B (26%) were the most common bleeding disorders. SVR12 results are shown in the below table by treatment regimen and genotype. The most frequently reported adverse events (>10%) were fatigue and headache; majority were mild or moderate in severity. One patient (<1%) discontinued LDV/SOF due to an adverse event and 11 patients (5%) experienced a serious adverse event. Hemarthrosis, muscle hemorrhage, epistaxis, hematoma, and hematuria were the only hemorrhagic events that occurred in >1 patient. Grade 3 or 4 laboratory abnormalities were infrequent with anemia and hyperbilirubinemia the most frequent Grade 3 laboratory abnormality consistent with RBV administration.
Conclusions:
SOF-based regimens led to high rates of SVR in genotype 1–5 HCV infected patients with bleeding disorders. SOF-based regimens were safe and well tolerated with no new toxicity specific to patients with bleeding disorders emerging
.
